
Special tests in physiotherapy are far more than routine checklists—they are precision tools that help clinicians uncover the root cause of a patient’s pain or dysfunction. By combining skilled observation, palpation, and targeted maneuvers, these tests provide invaluable insights into:
Joint integrity – detecting laxity, instability, or ligament damage
Muscle performance – assessing strength, endurance, and recruitment patterns
Neurological function – identifying nerve involvement or motor control deficits
Functional capacity – evaluating real-world movement patterns and balance

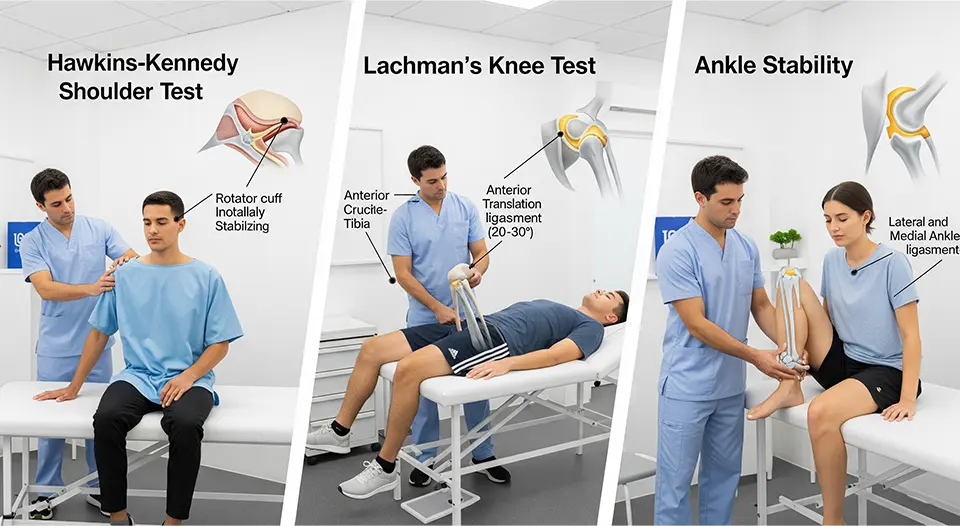
When it comes to the shoulder, special tests can differentiate between rotator cuff tears, impingement syndromes, labral lesions, biceps tendinopathy, and glenohumeral instability conditions that often share overlapping symptoms but require very different treatment approaches.
Similarly, in the realm of fall prevention and rehabilitation, standardized tools like the Berg Balance Scale (BBS) remain gold standards for objectively measuring a person’s static and dynamic stability. From elderly individuals at risk of falls to post-stroke patients relearning mobility, these tests provide measurable data that guide safe, effective rehabilitation plans.
This comprehensive guide is designed to be both educational and practical. Inside, you’ll find:
A complete list of shoulder special tests, each with its purpose, step-by-step instructions, and clinical interpretation tips.
A detailed overview of the Berg Balance Scale, including its 14 functional tasks and scoring system.
A downloadable quick-reference PDF, perfect for use in busy clinics, student study sessions, or home practice.
Whether you are a physiotherapist, sports rehab specialist, orthopaedic clinician, or physiotherapy student, this resource will equip you with evidence-based testing methods to improve diagnosis accuracy, enhance patient outcomes, and streamline your clinical workflow.
Special tests in physiotherapy are focused, evidence-based clinical procedures designed to assess the integrity, function, and stability of specific joints, muscles, ligaments, tendons, and neural structures. Unlike general movement screens which provide a broad overview of mobility and strength—special tests apply targeted mechanical stress, isolated muscle activation, or controlled positioning to reproduce symptoms, identify dysfunction, or confirm a suspected diagnosis.
These tests are a crucial part of orthopaedic assessment, as they allow physiotherapists to move from a general hypothesis to a specific, clinically supported conclusion. For example, while shoulder pain can stem from many causes, a sequence of shoulder impingement tests and rotator cuff special tests can help narrow down the exact structure at fault.
Main Categories of Special Tests
Orthopaedic Special Tests
Used to evaluate musculoskeletal injuries and joint-related conditions.Shoulder: Neer Impingement Test, Hawkins-Kennedy Test, Apprehension Test, Drop Arm Test
Knee: Lachman Test, Anterior Drawer Test, McMurray’s Test
Hip: FABER Test, FADIR Test, Thomas Test
Neurological Special Tests
Designed to assess nerve health, tension, and conduction.Upper Limb Tension Tests (ULTTs)
Straight Leg Raise (SLR) Test
Deep tendon reflex assessments
Functional Balance & Mobility Tests
Measure dynamic and static stability, gait, and fall risk.Berg Balance Scale (BBS)
Timed Up and Go (TUG) Test
Functional Reach Test
In modern physiotherapy practice, special tests are essential diagnostic and assessment tools that bridge the gap between a patient’s subjective symptoms and the objective clinical findings needed to create an effective treatment plan. They aren’t just about identifying the injured tissue—they influence the entire patient journey, from the first assessment to discharge.

1. Accurate Diagnosis & Differential Screening
Special tests allow clinicians to differentiate between multiple possible conditions that present with similar symptoms. For example, shoulder pain could stem from rotator cuff tendinopathy, labral tears, or impingement syndrome each requiring a different management approach. A well-chosen sequence of tests (e.g., Neer Impingement Test + Hawkins-Kennedy Test) can narrow the diagnosis quickly and accurately.
2. Determining Severity & Stage of Injury
Beyond identifying the structure involved, special tests help assess how severe the injury is whether it’s an acute partial tear, a chronic degenerative change, or a complete rupture. This distinction is crucial for setting safe rehabilitation timelines and managing patient expectations.
3. Guiding Evidence-Based Rehabilitation
By pinpointing the injured area and understanding the underlying mechanism, physiotherapists can design targeted, stage-appropriate treatment programs. For example:
Positive Apprehension Test → early stabilization and rotator cuff strengthening
Positive Drop Arm Test → progressive loading with careful avoidance of overhead stress in early rehab
4. Tracking Progress Over Time
Repeating specific tests during the course of treatment provides quantifiable benchmarks. Improvement in range of motion, strength, or pain response is a reliable indicator that the current rehab plan is working—or that adjustments are needed.
5. Enhancing Patient Education & Motivation
When patients see and feel the results of special tests—whether it’s the limitation on day one or the improvement weeks later—it builds trust, understanding, and engagement. It also makes abstract concepts (like “shoulder instability”) more tangible, improving compliance with home exercise programs.
6. Supporting Multidisciplinary Communication
Clear, test-based findings are valuable when collaborating with other healthcare professionals such as orthopedic surgeons, sports physicians, or occupational therapists. Test results provide a shared clinical language, ensuring consistent care across the team.
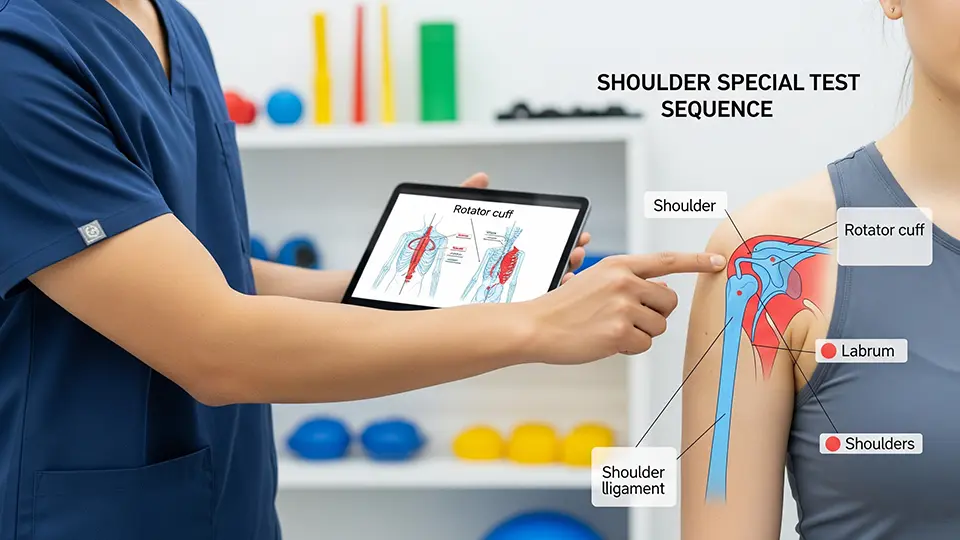
Shoulder special tests are manual orthopedic assessment techniques performed by physiotherapists, orthopedic surgeons, sports medicine clinicians, and other rehabilitation professionals to evaluate the integrity, stability, and function of specific structures within the shoulder complex.

These tests go beyond a general examination—they are targeted maneuvers designed to provoke symptoms, assess joint mechanics, and identify potential injuries such as:
Rotator cuff tears (e.g., supraspinatus tear detected via the Empty Can test)
Labral lesions (including SLAP tears and Bankart lesions)
Shoulder impingement syndromes (subacromial, internal, or coracoid impingement)
Glenohumeral instability or recurrent dislocations
Biceps tendon pathology (tendinitis, tenosynovitis, or tendon rupture)
Acromioclavicular (AC) joint injuries
Scapular dyskinesis contributing to pain or movement restriction
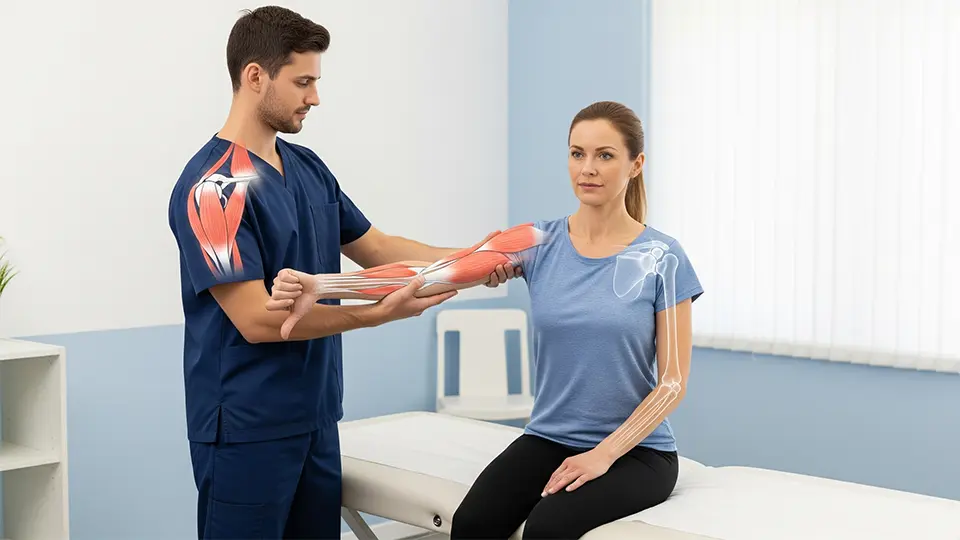
Shoulder pain is one of the most frequent musculoskeletal complaints worldwide, with causes ranging from sports injuries and overuse syndromes to age-related degeneration and postural dysfunction. Whether the patient is an overhead athlete, a manual laborer, or an older adult struggling with daily tasks, one thing is clear: a precise, evidence-based assessment is essential to guide effective treatment.
Shoulder special tests—also called orthopedic shoulder examination tests—play a central role in this process. They are structured, reproducible maneuvers designed to stress specific anatomical structures, helping clinicians identify the root cause of pain or dysfunction.
1. Neer Impingement Test

Purpose: Detects shoulder impingement syndrome, particularly involving the supraspinatus tendon or long head of biceps.
How to Perform:
Patient sits or stands.
Examiner stabilizes the scapula with one hand.
With the other hand, passively flex the patient’s arm forward in internal rotation until it reaches full elevation.
Positive Sign: Pain in the anterior or lateral shoulder during the end range indicates subacromial impingement.
Clinical Tip: A positive Neer combined with a positive Hawkins-Kennedy test increases diagnostic confidence.
2. Hawkins-Kennedy Test

Purpose: Screens for subacromial impingement of rotator cuff tendons under the coracoacromial arch.
How to Perform:
Patient seated.
Examiner flexes the shoulder to 90° and elbow to 90°.
Internally rotate the humerus.
Positive Sign: Pain or discomfort suggests impingement, especially of the supraspinatus tendon.
Clinical Tip: Often performed after Neer’s Test for a more complete impingement assessment.
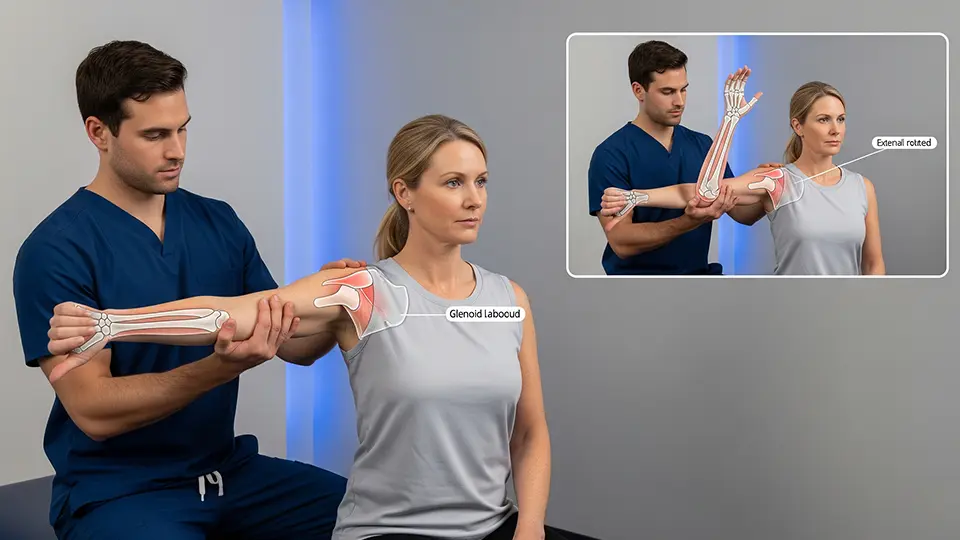
3. Apprehension Test (Anterior)

Purpose: Evaluates anterior shoulder instability due to capsulolabral injury or ligament laxity.
How to Perform:
Patient supine with shoulder abducted to 90° and elbow flexed to 90°.
Examiner slowly externally rotates the shoulder while applying gentle anterior pressure.
Positive Sign: Patient shows fear, apprehension, or resists further motion (rather than just pain).
Clinical Tip: Follow up with the Relocation Test to confirm instability vs. pain origin.
4. Speed’s Test

Purpose: Identifies biceps tendinopathy or superior labral lesions.
How to Perform:
Patient seated or standing with elbow extended and forearm supinated.
Examiner resists shoulder flexion at about 90°.
Positive Sign: Pain in the bicipital groove indicates pathology of the long head of biceps tendon.
Clinical Tip: Palpate the groove during the test to localize pain more accurately.
5. Empty Can Test (Jobe’s Test)
Purpose: Tests supraspinatus muscle and tendon integrity.
How to Perform:
Patient abducts arms to 90° in the scapular plane and internally rotates so thumbs point downward.
Examiner applies downward pressure while the patient resists.
Positive Sign: Weakness or pain indicates supraspinatus tear or tendinopathy.
Clinical Tip: Compare bilaterally to detect subtle strength deficits.
6. Lift-off Test

Purpose: Evaluates subscapularis muscle function.
How to Perform:
Patient places the back of their hand on the lower back.
Attempts to lift the hand away from the back against resistance.
Positive Sign: Inability to lift the hand off the back suggests subscapularis weakness or tear.
Clinical Tip: If patient can’t get into starting position due to limited mobility, try the Belly Press Test instead.
7. Sulcus Sign

Purpose: Indicates inferior glenohumeral instability or capsular laxity.
How to Perform:
Patient seated with arms relaxed.
Examiner pulls the arm downward at the elbow.
Positive Sign: Visible sulcus (gap) between the acromion and humeral head.
Clinical Tip: Grade the laxity (mild, moderate, severe) and compare both sides for baseline.
8. O’Brien’s Test (Active Compression Test)
Purpose: Detects SLAP lesions or AC joint pathology.
How to Perform:
Patient flexes shoulder to 90°, adducts 10–15°, and internally rotates (thumb down).
Examiner applies downward pressure while patient resists.
Repeat with palm up (external rotation).
Positive Sign: Pain with thumb down that reduces or disappears with palm up suggests labral lesion; pain over AC joint may indicate AC pathology.
Clinical Tip: Always interpret in context of other labral tests (Crank Test, Biceps Load Test).
While shoulder special tests focus on diagnosing joint stability, muscle integrity, and tendon health, the Berg Balance Scale (BBS) is a gold standard assessment tool used to evaluate a person’s functional balance abilities through 14 structured tasks that mirror real-life movements.

Who Benefits From the Berg Balance Scale?

The BBS is used across multiple patient populations, including:
Older adults – to screen for fall risk and guide fall-prevention programs.
Stroke survivors – to assess balance deficits and monitor neuro-rehabilitation gains.
Parkinson’s disease patients – to measure functional balance decline and progression.
Multiple sclerosis patients – to identify balance impairments linked to central nervous system changes.
Post-orthopedic surgery patients – e.g., after hip fracture or knee replacement, to evaluate safe mobility.
Vestibular disorder patients – to track balance recovery after vestibular rehab.
The 14 Tasks of the Berg Balance Scale (BBS)

| Task # | Description | Max Score |
|---|---|---|
| 1 | Sitting to standing | 4 |
| 2 | Standing unsupported | 4 |
| 3 | Sitting unsupported | 4 |
| 4 | Standing to sitting | 4 |
| 5 | Transfers | 4 |
| 6 | Standing with eyes closed | 4 |
| 7 | Standing with feet together | 4 |
| 8 | Reaching forward with outstretched arm | 4 |
| 9 | Retrieving object from floor | 4 |
| 10 | Turning to look behind | 4 |
| 11 | Turning 360 degrees | 4 |
| 12 | Placing alternate foot on stool | 4 |
| 13 | Standing with one foot in front | 4 |
| 14 | Standing on one leg | 4 |
Total Possible Score: 56 points
Scoring and Interpretation
41–56 points: Low fall risk
21–40 points: Medium fall risk
0–20 points: High fall risk
Lower scores indicate poorer balance control and higher likelihood of falls.
Advantages of the Berg Balance Scale (BBS)
The Berg Balance Scale has earned its place as one of the most trusted functional balance assessments in clinical practice—not just because it’s widely recognized, but because it delivers practical, evidence-based benefits for both therapists and patients.










1 thought on “Special Tests in Physiotherapy: Shoulder Special Test & the Berg Balance Scale – Complete Guide with Scores, Instructions & PDF”
Very interesting info !Perfect just what I was searching for! “The only limit to our realization of tomorrow will be our doubts about reality.” by Franklin Delano Roosevelt.